Commentary
There is no better time for the countries of Southeast Asia to reconsider their energy security than during this latest crisis.
Gita Wirjawan

Source: Getty
Japan's experience at the forefront of demographic change can provide lessons to other advanced industrialized economies in search of the appropriate policy response to aging societies.
In nearly all advanced industrialized economies, populations are graying—the result of improved access to quality health care and nutrition which contribute to longevity, the postwar baby boom, and lower birth rates, among other factors. Unprecedented gains from this longevity—more time to spend with loved ones and to achieve personal goals—should be celebrated. But from a policy perspective, the trend is worrying. Most governments are ill-prepared to deal with the economic and social consequences of aging populations. In the coming years, as advanced-country policymakers seek to provide care to the elderly that is both high quality and financially sustainable, Japan—which has the oldest society in the world, with nearly a quarter of its population over sixty-five years old, and is the first to confront the aging challenge—may offer some useful lessons.
Japan was not always at the forefront of demographic change. In the late 1960s, just 6 percent of the population was over sixty-five—a share surpassed by Russia, the United States, and much of Western Europe. Between 1970 and 1980, however, as Japan’s economy reached the late stages of industrialization, its society began to age faster than any other. In 2005, Japan officially overtook Italy to become the oldest society in the world (see figure).

In the 1990s, policymakers realized that they would have to transform the nation’s approach to eldercare. Before 2000, aging Japanese received care in one of three settings: the welfare system, the health care system, or their own home. But each was accompanied by serious problems. Accessing the welfare system involved a tedious application process; services were scarce; and users faced the stigma of receiving a “handout.” Universal health coverage with minimal copayments provided aging Japanese with a second option of receiving care through the health care system. But the per capita cost of hospital beds was (and still is) very expensive. And the traditional system of receiving care at home from family members often proved inadequate, as the caregivers aged and found themselves unprepared to address the range of complex physical and psychological issues that the elderly face.
The public long-term care insurance (LTCI) program that Japan crafted and launched in 2000 addressed this fragmentation by consolidating services for the aging into one program. Through the program, an elderly Japanese would be certified as eligible for LTCI and assigned a qualified “care manager.” The care manager would be responsible for assembling a care plan for the user and determining, on the basis of his or her physical and mental health, the appropriate mix of covered services that he or she would need to access. Over the past decade, LTCI has improved quality of life for the elderly, reduced the caregiving burden on relatives, and remained financially sustainable.
The Japanese LTCI system has four main features. First, it relies on “hybrid” financing: social insurance premiums, taxes, and user copayments. The insurance premium linked to use of the program was needed to eliminate the stigma attached to the means-tested welfare system open to anyone in need. Taxes, meanwhile, keep premiums down and are used to subsidize LTCI provision in poorer municipalities.
Second, only those over forty years old are charged the premium, and eligibility for benefits is restricted accordingly. The government attempted to include those younger than forty to provide additional support for disabled youth and strengthen LTCI’s financial base, but this idea was rejected due to the minimal health risks that the under-forty face. A compromise was struck instead: those over forty but under sixty-five would benefit from the program because it would ease their caregiving burden.
Third, LTCI does not provide a cash benefit. Women’s rights groups argued that a cash benefit would not free wives, daughters, and daughters-in-law from their caretaking burden. Even providing a choice between in-kind and cash benefits would put pressure on women in a male-oriented society to stay at home and provide care, they maintained. Because LTCI takes the form of an in-kind system, it has stimulated demand for care services and created a new market and new jobs in the local economy. 1
Fourth and most important, municipalities serve as insurers in the LTCI system, creating an incentive for them to keep costs low. They have responded by establishing and maintaining an efficient caregiving infrastructure and promoting preventative care, including physical exercise as well as opportunities for the elderly to socialize, and home care, which is generally less expensive than institutionalized care.
The comprehensive community care (CCC) system, which the LTCI system will eventually support, can be viewed as a more advanced version of “integrated care.” Three of the elements upon which the CCC system is based are described in a World Health Organization report: preventative care for the promotion of physical and mental health; medical care for patients in an acute stage of illness; and long-term care for patients suffering from terminal illnesses or chronic conditions. CCC includes two additional elements: living support services and residential arrangements, so that the elderly can continue to live in their own communities.
From a financial standpoint, enabling the elderly to continue living at home is a relative bargain. The public pension system has matured to the point where the financial condition of the elderly is comparable to that of the young.2With modest home care services, many of the elderly can and have been able to stay in their own homes—which not only is a less expensive arrangement than care in most institutional settings but has also been shown to help the elderly maintain their quality of life.
The government’s goal is to establish CCC—that is, provide access to these five services—within any potential recipient’s “daily living zone” (defined as within thirty minutes’ walking distance) by 2025, when the share of the population over sixty-five will reach almost 30 percent.
The aim of long-term care insurance and comprehensive community care is, respectively, to enable the elderly to maintain stable consumption and to live independent lives for as long as possible. Younger Japanese also benefit from the system because they are freed from the responsibility of supporting their parents after retirement, including covering unexpected medical or nursing costs, by relying mostly or entirely on their own earnings.
To be sure, relying too heavily on intergenerational support—that is, taxes on and social security contributions from younger generations—could erode the social compact underlying LTCI. This could heighten perceptions of inequality within the broader social security system among younger Japanese, who came of age as Japan’s economy stagnated. Additional cost-containment measures, such as increasing LTCI copayments and better matching needs to covered services, may need to be implemented. Further, even as LTCI tends to the elderly, services for younger, working-age Japanese—helping them find decent jobs, encouraging marriage, and facilitating childrearing—should be strengthened.
As is the case in most other advanced industrialized economies, providing quality care to the elderly while arranging for sustainable financing will be the most significant challenge facing LTCI and the achievement of CCC. LTCI spending has increased as the system has matured. The total cost of benefits increased between 2005 and 2009 from ¥5.8 trillion ($72.5 billion) to ¥6.9 trillion ($86.3 billion). Though cost-containment measures, including a controlled fee schedule and a ceiling on the availability of covered services based on the level of care a patient needs, are included in the system, the average monthly premium for the elderly is ¥4,972 ($62.2) for fiscal years 2012–14, a 22 percent increase from fiscal years 2006–08.
The cost of LTCI will increase further in the future as Japan continues to age but there is reason to believe that the program is on a financially sustainable path. The formula for total social spending will restrain future growth in public pension expenditures, enabling LTCI costs to rise without significantly raising the overall expense of the social safety net. Between fiscal year 2012 and fiscal year 2025, social security expenditures are projected to increase modestly from 22.8 percent to 24.4 percent of GDP. The Japanese cabinet is also considering measures to shore up the finances of the program, including increasing Japan’s consumption tax. Finally, the political will exists to make difficult fiscal choices in order to support LTCI—a program that was designed to care for a quarter of Japan’s population and, in fact, benefits a far-larger share.
Taichi Ono is currently assigned to the Pension Bureau of the Ministry of Health, Labour, and Welfare in Japan. He was formerly a professor at the University of Tokyo’s Graduate School of Public Policy.
[1].About 1.34 million people worked for LTCI-financed service providers in 2009, which means that about 0.8 million jobs have been created since 2000.
[2].In 2010, according to data from the Ministry of Health, Labor, and Welfare, average annual per capita income for households headed by an individual sixty-five or over was about $24,000, as compared to $26,000 for all households. In 2010, public pensions accounted for over 70 percent of total income for the average elderly household. According to 2010 cabinet data, Japanese elderly are less likely to perceive themselves as having economic problems: 55.5 percent of the Japanese responded as “having no economic worries at all.” This figure was lower than in Sweden (58.4 percent), but larger than in Germany (38.4 percent), the United States (31.2 percent), and Korea (11.2 percent).
Taichi Ono
Carnegie does not take institutional positions on public policy issues; the views represented herein are those of the author(s) and do not necessarily reflect the views of Carnegie, its staff, or its trustees.
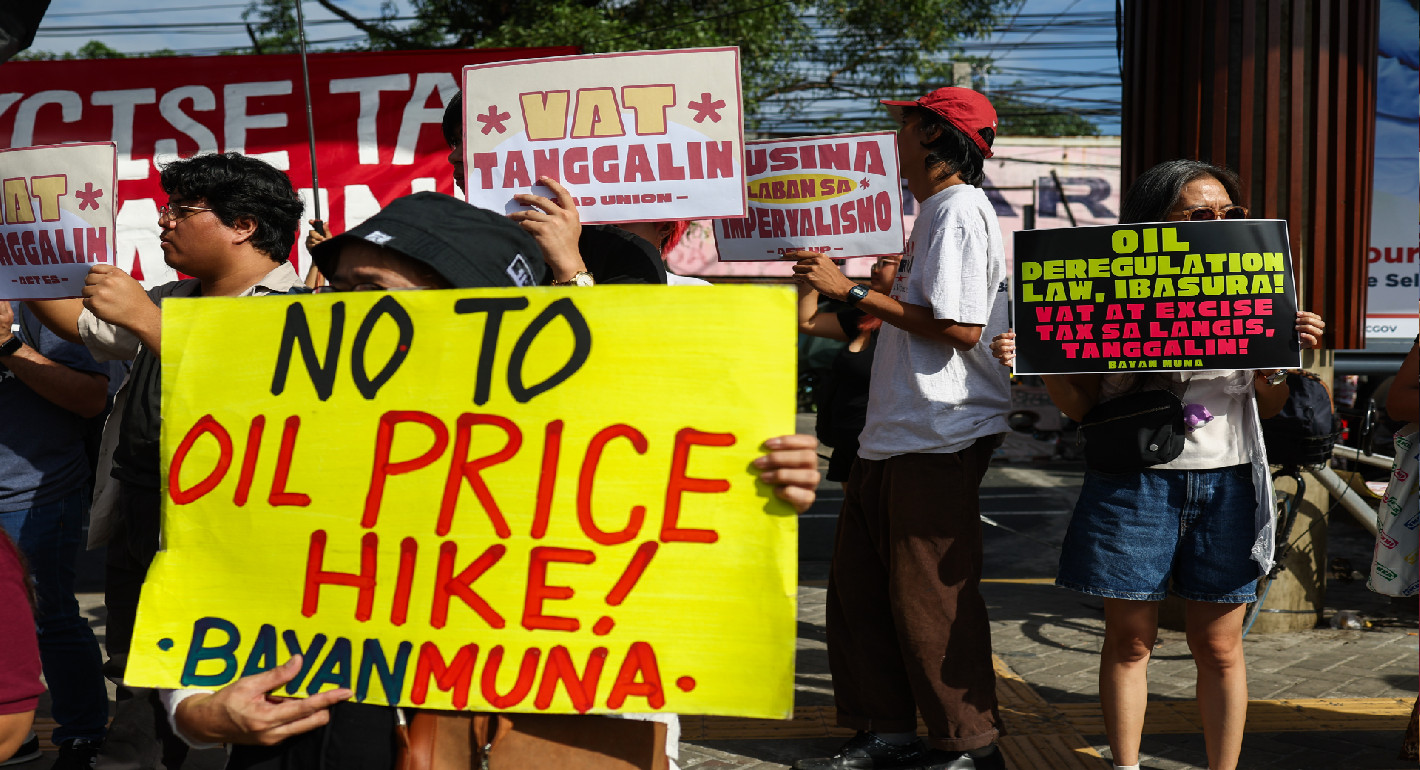
There is no better time for the countries of Southeast Asia to reconsider their energy security than during this latest crisis.
Gita Wirjawan

As conflict in the Middle East drives up fuel costs across Asia, Indonesia faces difficult policy trade-offs over subsidies, inflation, and fiscal credibility. President Prabowo’s personalized governance style may make these hard choices even harder to navigate.

Sana Jaffrey

The United States ignores the region’s lived experience—and the tough political and social trade-offs the war has produced—at its peril.

Evan A. Feigenbaum

The GDP measure is an attempt to measure value creation in an economy. This measure, however, can vary greatly between economies that have disciplinary mechanisms that force them to recognize investment losses quickly and economies that don’t, and can postpone this recognition for many years.

Michael Pettis

As the Iran war shocks oil prices, countries that have invested in renewables, EVs, and battery development since the 2022 Russian invasion of Ukraine are seeing the value of their investments.

Noah Gordon